
The Reason for 4 Gland Parathyroid Assessment
If you are diagnosed with hyperparathyroidism, then at least one of your four parathyroid glands is producing too much parathyroid hormone (PTH). The majority of patients will have a benign hormone producing tumor in one parathyroid gland, however, 15–25% of patients will have more than one abnormal parathyroid. The chance of having more then one abnormal gland actually increases the lower the PTH level is (this seems counter-intuitive but it is very true). In fact, when the PTH is less then 100 pg/ml the chance of having more then one abnormal gland increase from 15% to 25%. To ensure that a minimally invasive parathyroidectomy is a success, Dr. Larian performs an individualized 4 gland parathyroid assessment on every patient. This is necessary to ensure parathyroid surgery is successful and to prevent the patient from going through the surgery and wake up still having hyperparathyroidism.
Unfortunately there is no such thing as a one-size-fits-all approach to parathyroid disease diagnosis and treatment. By working with Dr. Larian, patients receive individualized support and care from a highly trained and experienced parathyroid physician & surgeon. Dr. Larian works closely with each hyperparathyroid patient to ensure proper evaluation. Dr. Larian will do everything possible to identify the abnormal parathyroid gland or glands, he then offers a personalized treatment plan to his patients.


4 Gland Parathyroid Assessment Tools
There are a variety of ways to evaluate all 4 parathyroid glands. Years ago the only available tool was to look at the 4 glands in surgery (4 gland bilateral exploration) to make an assessment whether they are abnormal or not. As our understanding of the disease improved and the tools we use in surgery have improved, parathyroid surgeons have changed to evaluating the function of the parathyroid glands during surgery rather then just how the glands look. Historically 4 gland exploration was the first technique, followed by radio guided parathyroid surgery, and the latest technique is parathyroidectomy with rapid intra-operative PTH testing. As a parathyroid surgeon, I find that I need to know, understand and at times use one or more of these techniques to be successful in treating the patient. I’ll discuss the techniques and their pros and cons.
4 Gland Exploration (Bilateral Neck Exploration)
“Since the first parathyroidectomy performed in 1925 by Dr. Felix Mandl of Vienna, bilateral neck exploration (BNE) by an experienced surgeon has been the gold standard with operative success rates of >95% in patients with primary hyperparathyroidism”. This technique had been the only surgical technique to treat hyperparathyroidism for 70 years, until the late 1990’s. It involves making an incision in the middle of the neck, and looking behind the thyroid on both sides of the neck and finding all 4 parathyroid glands, visually inspecting them and then removing the glands that appear visibly abnormal, and leaving the ones in place that appear normal. This is often done in combination with sending a portion of all 4 parathyroid glands to the pathologist to look at during the surgery to help decide which glands both physically and under the microscope look abnormal to be removed.
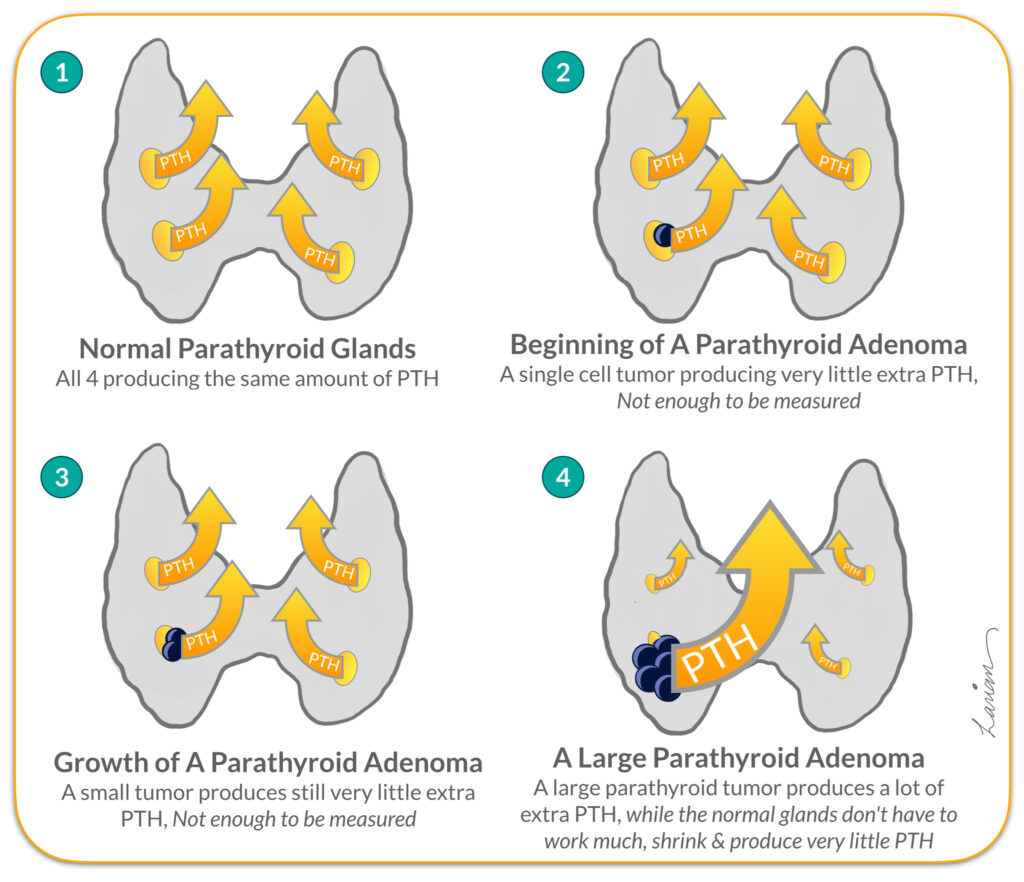
On first glance this looks like a very sensible option, except that the amount of hormone a gland produces does not always correlate with it’s size, or color, and abnormal parathyroid cells look exactly the same as normal ones under the microscope. Add to this problem, an even more problematic issue is that as a parathyroid tumor (adenoma) gets bigger and produces more parathyroid hormone (PTH) the remaining normal glands that see the calcium rising stop working, therefore the normal glands shrink and get smaller and smaller. These smaller normal parathyroid glands can be harder to find, however in the hands of an expert parathyroid surgeon that is not a problem experience and expertise can’t overcome. The real problem is that the smaller glands will have smaller blood vessels and therefore in the process of looking for these smaller normal glands the chance of causing injury to the gland and more likely to the blood

vessel feeding the gland is higher. So again the reason a bilateral neck exploration is done is that at most 25% of people with hyperparathyroidism will have more then one abnormal gland, and by looking at both sides you will find the additional abnormal glands. However, 75% (a majority of patients) have only one abnormal gland and doing a bilateral neck exploration on every patient unnecessarily risks compromising and damaging their normal healthy parathyroid glands, and potentially causing permanent hypoparathyroidism. Essentially, bilateral neck exploration is an over-aggressive operation for 75% of people with hyperparathyroidism who have only one abnormal gland. In the old era, and in areas & countries where the modern parathyroid localization scans and surgical technology is not available it may still be the only option.
Another reason not to do bilateral exploration on everybody is that by operating on both sides, the risks of surgery will increase. The Recurrent Laryngeal Nerve (RLN) that goes to the voice box and controls the vocal cords on each side goes behind the thyroid and in between the upper and lower parathyroids, so by exploring both sides of the neck you risk injuring both nerves as opposed just exploring one side and risking only potential injury to one nerve. Additionally, every area of the body under the surface that is touched or explored will create scarring; this is the bodies natural reaction to surgery. If that person needs surgery in that area again, the surgeon will have to go through scar tissue to do the second surgery. Risk of injury to RLN and normal parathyroid glands is significantly higher when a second surgery becomes necessary. A very good question is “why would someone need a second surgery?” (1) If the person develops a nodule or cancer in the thyroid that may need to be removed. (2) If the person develops another parathyroid adenoma years later (happens in less then 10% people with hyperparathyroidism due to an adenoma).
Today, 4 gland exploration (Bilateral Neck Exploration) is used when multiple different localization scans (ultrasound, 4D CT scan, Sestamibi etc.) are negative, and are not able to identify which gland is enlarged or overactive, increasing the likelihood that the person may have all 4 glands be abnormal (parathyroid hyperplasia) which means all 4 parathyroid glands need to be visually


inspected and a subtotal parathyroidectomy may be considered. Or when during surgery, after removal of one enlarged parathyroid gland (the one seen on scans before surgery) the intra-operative rapid PTH levels are still high, indicating that there are more over-active glands that need to be removed.
Minimally Invasive Radio Guided Parathyroidectomy
Minimally invasive radio-guided parathyroid surgery involves the use of a small injection of Tc-99m sestamibi nuclear material on the morning of surgery, at the same time doing a sestamibi scan to visualize which gland is concentrating the radioactive material. Tc-99m sestamibi will concentrates in the Mitochondria (engine of cells) of abnormal parathyroid glands that are overworking, making it easier for a surgeon to determine their location and level of activity. In the operating room, the surgeon could use a probe that measures radioactivity (Gamma Probe) either on the skin, inside the wound, or on the piece of tissue (though to be parathyroid) removed from the patient. This was first described by Dr.’s Martinez & Martin in 1995 at Ohio State University, and then refined and popularized by Dr.’s Norman & Chheda in 1997. It was a revolutionary change in the way parathyroid surgery was being done because now there was a way to potentially both locate the abnormal gland & measure it’s level of activity.
Most parathyroid surgeons were very excited and a lot, including me began to use this technology. Not only was radio-guided surgery pointing the surgeon to the overactive gland, it was allowing the surgeons to use a small incision and only look for the abnormal glands and not disturb the normal glands, which is the true essence of the term minimally invasive parathyroidectomy. Fortunately, both the sestamibi scan and the Gamma probe were readily available at my hospital. However, for surgeons with expertise in parathyroid surgery using the probe to find the parathyroids was not as necessary as checking the activity of the gland. Unfortunately, in time we found that the sestamibi nuclear material is not always specific for parathyroids, and can accumulate in thyroid nodules, thymus, and other types of tissue in the neck and therefore there was a degree of unreliability with this technology. Additionally, not all overactive parathyroids were apparent with this technique. So sometimes the Gamma probe would say a tissue is overactive parathyroid & it wasn’t parathyroid at all, and sometimes it would say the parathyroid is normal & in fact it was an over-active parathyroid. This degree of unreliability led to parathyroidectomy failures, and persistence of hyperparathyroidism. By mid 2000’s most surgeons decided to no longer use radio-guided surgery and look for more accurate methods, while others wanted to improve radio-guided surgery by combining it with bilateral neck exploration (which as explained in the section above, has unnecessary increased risks along with no longer being minimally invasive but rather maximally invasive), or rapid intra-operative PTH testing.


Minimally Invasive Parathyroid & Intra-Operative PTH Testing
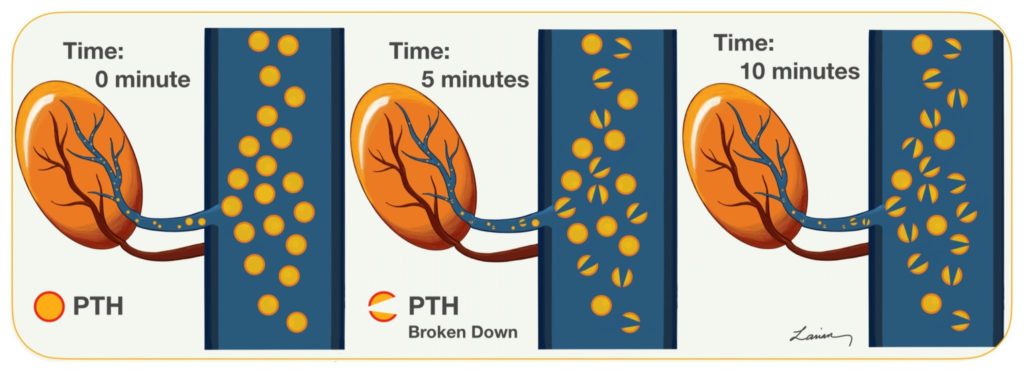
Parathyroid Hormone or PTH is released into the blood by the parathyroid gland in response to low calcium. PTH has a very short half life of about 5 minutes, which means that half of the PTH produced at this moment is broken down and will not work in 5 minutes, by 10 minutes 75% is broken down.
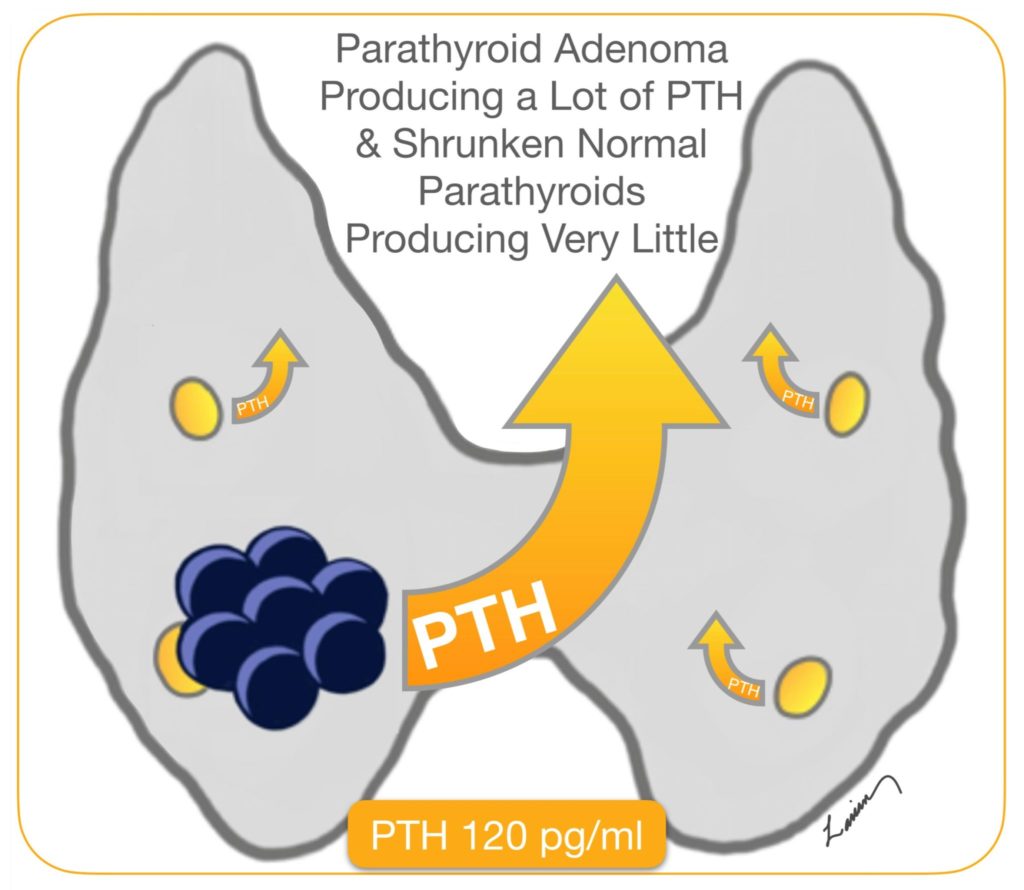
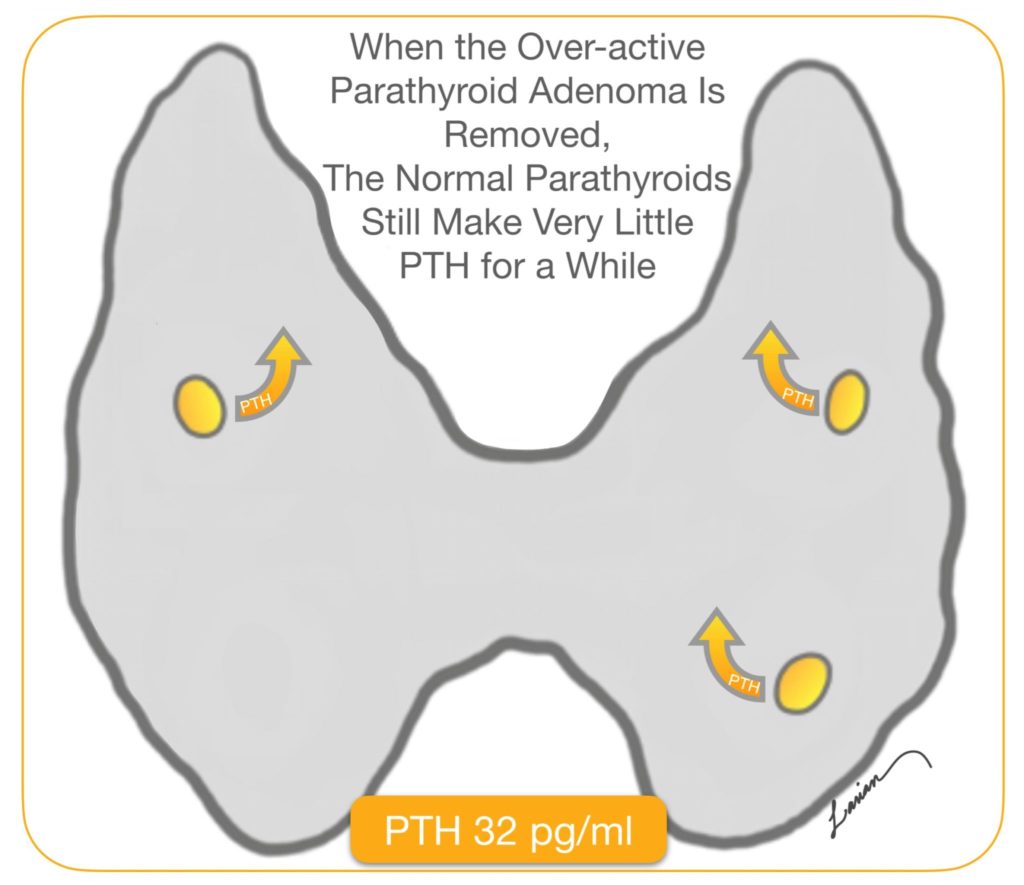
In 1990’s a brilliant physician Dr. George Irvin at the University of Miami realized he could use this information to help in surgery. He understood that when a parathyroid adenoma is working hard and producing a lot of hormone (PTH), then the remaining normal glands would not need to work. These none working parathyroid glands shrink, get smaller (atrophy), and produce very little PTH. When the parathyroid adenoma is removed in surgery, the normal smaller parathyroid glands that have not been doing much work for a long time will still make very little PTH. It takes a few weeks before these normal glands go back to working normally.

The problem had been up to this point that the laboratory test to check for PTH took several hours to days to give results, which made it not useful during surgery. However, Dr. Irvin had at his hospital a rapid PTH machine which he could get results in 30 minutes. This was also a revolutionary change in parathyroid surgery, because with rapid PTH testing you didn’t have to inject a foreign radioactive material to check the level of activity of the parathyroids, but rather the surgeon could just check the amount of PTH hormone being produced during surgery to know if there are still over-active parathyroid glands.
Minimally invasive parathyroidectomy with rapid intraoperative PTH testing was very exciting, because it could truly let surgeons be minimally invasive (meaning in surgery only look for & disturb the abnormal gland), and check how active the other 3 glands were by directly checking the blood levels of PTH, the hormone causing all the problems in hyperparathyroidism without having to look for them visually, disturb them and potentially damage them. Over time surgeons realized intraoperative PTH testing was even more useful then originally anticipated; not only could the surgeon confirm the the success of surgery once the abnormal gland or glands had been removed, they could also make sure the remaining glands were still working. The combination of minimally invasive parathyroidectomy and intraoperative PTH testing has proven to be very reliable with 99% cure rates being reported with this approach. While at the same time minimizing risks because you explore more then one area only when PTH levels don’t come down appropriately (which happens less then 25% of cases). So the 75% of people who have a single adenoma don’t need to undergo a surgery that risks damage to the nerves, blood vessels, thyroid and parathyroids on both sides.
However, there was a clear limitation to this technology; the rapid PTH testing machine was not available at most hospitals. So most parathyroid surgeons did not have access to it. And it took years for surgeons that were dedicated to doing parathyroid surgery to convince their hospitals to purchase these expensive machines and learn how to use intra-operative rapid PTH testing properly. In my case this happened in 2005. Additionally, it required the surgeon to change the way they performed the surgery: (1) they had to have more exact localization studies then the sestamibi nuclear scan alone to find the enlarged parathyroid gland, and (2) the surgery took longer because they had to wait an additional 30 minutes during surgery to get blood PTH results during which they had to mostly sit patiently to see if the numbers came to down appropriately before they were confident the parathyroid they had removed was the only one that was overworking. Not all surgeons had that kind of patience, and if the PTH level did not come down then they had to continue operating and keep testing which could make the surgery much longer. It required parathyroid surgeons to make a complete shift in the way they did parathyroid surgery.
Examples of Customized 4 Gland Parathyroid Assessment
To give patients an idea of how Dr. Larian customizes every parathyroid surgery with an individualized 4 gland parathyroid assessment, here are a few examples of different surgical approaches:
Example 1 – MINIMALLY INVASIVE PARATHYROIDECTOMY with ONE SIDED FOCUSED PARATHYROID REMOVAL & PTH TESTING
A 62 year old woman with symptomatic hyperparathyroidism, and an enlarged right superior parathyroid seen on ultrasound. The remaining parathyroid glands were not visible. The Calcium level were usually around upper 10’s mg/dL (normal range 8.8-10.2 mg/dL), and PTH around 70-80’s pg/ml (normal range 15-65 pg/ml).
")
A sample of blood was obtained before the surgery was started and tested for PTH, the amount was 86 pg/ml. This surgery was performed under local anesthesia, with a slight amount of sedation. The right recurrent laryngeal nerve RLN (voice box nerve) was identified and right next to it the right superior parathyroid was identified and removed, 10 minutes later a sample of blood was tested for PTH which came back at 32. This is more then a 50% reduction in PTH, and it indicates the remaining glands are dormant and not producing much PTH, and also that the surgery was successful. The pathology report shows a hypercellular parathyroid with a rim of normal parathyroid tissue, indicative of a parathyroid adenoma.

Example 2 – MINIMALLY INVASIVE PARATHYROIDECTOMY with LIMITED BILATERAL EXPLORATION & PTH TESTING
54 year old man with kidney stones and hyperparathyroidism symptoms. His calcium have been in the upper 10’s and lower 11’s, with PTH levels that have gradually become higher. Ultrasound showed a benign appearing thyroid nodule on the left. Prior A 4D parathyroid CT scan was done to get further clarification, and it showed an enlarged parathyroid on the right side superiorly & a possible lesion deep to the thyroid nodule inferiorly on the left side.

PTH level before the start of surgery was 87 pg/ml, and during surgery before removal of the right upper gland was 92 pg/ml. After finding the right recurrent laryngeal nerve and protecting it, the right upper parathyroid was removed the PTH came down to 64 pg/ml. Since this is less then a 50% reduction in PTH, it means there is at least one more overactive gland. Since the scans had indicated a second target on the left lower side, that was the next area to be looked at.

The left recurrent laryngeal nerve was was found immediately underneath the abnormal parathyroid and was gently separated from the enlarged parathyroid (not quite as large as the first one). 10 minutes after the left lower parathyroid was removed the PTH was tested again and came down to 12 pg/ml. Indicating the remaining 2 parathyroid glands were functioning normally and don’t need to be found, disturbed or removed. The thyroid nodule on the left side was also removed and on final pathology was also benign thyroid nodule (that no longer needs to be monitored for growth with repeated ultrasounds).

Both parathyroids on final pathology report were densely cellular (hypercerllular) and had a rim of normal parathyroid tissue, confirming that they were parathyroid adenomas & not hyperplasia.
Example 3 – MINIMALLY INVASIVE PARATHYROIDECTOMY with COMPREHENSIVE BILATERAL EXPLORATION & PTH TESTING
A 43 year old woman with chronic pain and osteoporosis. Calcium levels have slowly been rising up over the past decade, and have been above normal range over the past 4 years. PTH levels are also gradually increasing. Sestamibi and 4D parathyroid CT scans were both negative. Ultrasound done in the office indicated possible enlarged parathyroids in the left upper and right lower areas. She does have a family history of an aunt with untreated hypercalcemia. All together there was a higher degree of suspicion that this may represent parathyroid hyperplasia.

PTH levels obtained before surgery was 82 pg/ml. The left upper parathyroid was to be identified first as it was the largest on ultrasound and potentially an adenoma. The left recurrent laryngeal nerve was identified and could be seen going over the left upper parathyroid, the nerve was then gently separated from the the parathyroid gland. The left upper parathyroid was clearly enlarged, brownish in color and plump, as such it was removed and PTH levels checked after 10 minutes which showed only minimal reduction down to 67 pg/ml.
The exploration continued and the left lower parathyroid was identified immediately next to the nerve; it was slightly enlarged. Attention was directed to the right side, the lower and upper parathyroids were found after identifying and protecting the voice box nerve (Recurrent Laryangeal Nerve). The right lower parathyroid was similar in size to the parathyroid glands on the left. The right upper parathyroid was much smaller and farther away from the nerve. The left lower and right lower parathyroids were also removed and PTH levels tested again; the number came down to 12 pg/ml indicating not only the success of the procedure but the fact the right upper parathyroid was functioning adequately.

Example 4 – MINIMALLY INVASIVE RADIOGUIDED PARATHYROIDECTOMY with ONE SIDED FOCUSED PARATHYROID REMOVAL IN THE UPPER CHEST & PTH TESTING
A 64 year old woman with history of hyperparathyroidism causing severe symptoms and osteoporosis. The calcium levels had been high in the upper 11’s and low 12’s for over 2 years. Her PTH levels had been continuously coming up and was in the 200 range. The work up included an ultrasound which did not show any enlarged parathyroid in the neck. A 4D CT scan was done which showed an enlarged parathyroid in the upper chest close to the blood vessels coming from the heart.
The decision was made to attempt to remove the parathyroid through the neck rather then making an incision on the chest or splitting the chest bone. A sestamibi scan was done the morning of surgery which also showed the overactive parathyroid in the chest, and the patient was taken to the operating. PTH level immediately before surgery was 211, and during surgery before removing the tumor it was 237.

A Gamma probe (radioguidance) was used to help locate the parathyroid in the chest, since there is limited space for access through the neck. Once the tumor was located and removed PTH levels were checked and showed a quick drop to 46, which meant the other 3 glands were normal and did not need to be identified, or removed.
FAQ (Frequently Asked Questions)
Yes, it is crucial in helping the surgeon be certain that they were able to cure/treat the hyperparathyroid condition adequately and appropriately before the surgery is finished. Hyperparathyroidism is a very unusual disease because more then one gland can be abnormal and yet the symptoms are the same if one gland or all 4 glands are abnormal. And all the abnormal glands may or may not be visible on scans, so when your surgeon goes into the operating room thinking based on the scan that there is only one abnormal gland, more could be diseased and 4 gland assessment techniques alert the surgeon.
As outlined above each technique has it’s own advantages and risks. It is up to your surgeon to decide and discuss with you what is most appropriate in your circumstance. This is a very important discussion that you as a patient should be informed and prepared to have with your surgeon. Knowing all the potential risks & benefits will allow you to have a meaningful conversation. If you believe the risk of a particular technique is not necessary for your particular case then please discuss that.
Extremely rarely I perform a parathyroidectomy without 4 gland assessment. It is in the setting of very ill patient (severe lung or heart disease) that is being deeply effected by hyperparathyroidism, but surgery is very risky for their heart or lungs. The patient must have a reliable localization scan. Under the circumstances a parathyroidectomy would be done under local anesthesia so as to not put pressure on the heart.
You have to ask the surgeon if they do it and which technique they use. Most physicians don’t have it on their website, because it is a complicated subject to explain.
The amount of time required to complete a 4 gland assessment varies based on the number of abnormal parathyroid glands, how many of the abnormal glands are seen on scans, and the technique used. It could be as short as 30 minutes (15 minutes to remove the abnormal gland, and 15-30 minutes to get rapid PTH results) in most cases, to a few hours for revision parathyroidectomy.
Hyperparathyroidism can be very challenging to diagnose and treat. Many surgeons, as they go through their careers and treat hyperparathyroidism, will struggle with complex parathyroid cases. They will try many different techniques, until they find one that works best in their hands. And they will continue to always use that technique. Others are versatile and continually change and evolve their technique.
The group of parathyroid expert reviewed all the available research and stated that the Gamma probe in radio-guided parathyroidectomy added very little additional information to the sestamibi scan, which is different then advising against it. More importantly, it was a turning point for those who were using it solely, to make a change. Most groups who are currently using the probe have made changes to evolve the surgery, and some use intra-operative PTH testing along with radio-guidance. I unfortunately find that is helpful to me in very rare cases.
Since sestamibi nuclear material is attracted to the engine of the overactive cells, rather then parathyroid cells or parathyroid hormone specifically, it can be attracted to other types of cells that may be active. So in cases where there are nodules in the thyroid gland, the nuclear material may accumulate in the nodule which may mislead the surgeon. Thymus gland which is close by and salivary tissue which is further up in the neck can also accumulate the nuclear material. So basically good parathyroid surgeons are not good because they use the probe but rather that they are skilled surgeons.
Additionally, the level of attraction of parathyroid cells for sestamibi is not the same for everyone, so an overactive gland may not show activity to the probe not because its not producing excess PTH but rather because it does not accumulate sestamibi nuclear material as much as expected.
No technique is without its potential downsides. I’ve been using the rapid PTH testing since mid 2000’s and have found over the years that the potential failures with this technique occurs in patients that have kidney problems and obesity. The kidney filters 30% of the PTH in the blood and if the it’s not functioning properly then the PTH level after the parathyroid adenoma is removed may not drop by the 50% criteria. Obesity also affects the breakdown of PTH and may make it longer. In both these scenarios, the surgeon has to keep this in mind when looking at intra-operative-operative PTH level changes.
Failure of parathyroid surgery has been reported to be anywhere between 1-15%. I would say that on the upper side (5-15% failure rate) has more to do with the surgeon’s lack of experience (surgeon’s doing less then 50 cases a year), and most parathyroid surgeries are done by surgeons that only do a few cases a year.
Most centers consider recurrence in the first 6 months after surgery to be a failure, and if the PTH and calcium rises up in month 7 then that is not considered failure of surgery. I report my failure to be around 3%, but that is because I consider my long term recurrence as part of that. So if a person comes back several years after surgery and has another adenoma or hyperplasia I would include that as part of failure statistics. This makes most sense to me, and I think the best for patients to be able to understand.
Failures fall into two categories: (1.) ones where the abnormal parathyroid was not found, and (2.) ones where an abnormal gland or glands were removed but the person continues to have hyperparathyroidism.

The poor patients that fall into this group generally have surgery done by a surgeon that is less experienced and depends on low quality localization scan, or the abnormal gland is in an ectopic location. By ectopic I mean in an unusual location such as the chest or throat and may have not been visible or was missed on the scan; unfortunately it does happen, at times, that when a patient comes to me after a failed surgery elsewhere I review their original scan and can see the parathyroid that was missed.

Over the past 2 decades of performing parathyroidectomy, I have found several reasons for failure for myself, and when I perform reversion parathyroidectomy for the failure of other very experienced parathyroid surgeons. There are generally 2 categories:

There are times when there are 2 parathyroid adenomas, one that is very large and actively producing PTH to baring the calcium level to 12.2 mg/dL, and one that is very small (microscopic), inside the normal parathyroid gland and producing very minimal amounts of PTH at this point. So when the larger one is removed, the smaller parathyroid adenoma is too small to be visible to the naked eye, is working too little yet to be active on radioguidance, and producing too little PTH to be noticed on intraoperative PTH testing.
The other scenario, which is even more common, happens when there is a parathyroid adenoma growing on the background of parathyroid hyperplasia. In this circumstance, when the adenoma is actively working to bring the calcium level up to 11.7 mg/dL, the other hyperplastic parathyroid glands may be somewhat suppressed and not producing much PTH; even though they are anbormal, they are not as active as the adenoma and cannot essentially compete. So they may appear small in size, not be active on Sestamib scan or radioguidance, and not produce enough PTH to be noticed on intraoperative PTH testing.

One that seems promising is near-infrared auto-fluorescence, which depends on the excitation (fluorescence) by light of parathyroid glands in the near infrared spectrum being different from thyroid and other tissues in the neck. Although it holds promise, as of yet it has not been shown to be able to distinguish between a normal and abnormal parathyroid reliably. Hopefully it can be made useful in the future.
Parathyroid disease is a complex medical condition, one that requires expert support to treat. Dr. Larian, considers every person’s case as individual and unique and will devise a surgical plan for them individually. They will personally evaluated before surgery, the most appropriate scan for their individual case will be done and reviewed personally by Dr. Larian, and they will have a treatment plan designed for their circumstance. Everything will be explained in detail before surgery. Every patient will have a 4 gland assessment by the technique most appropriate for them, and will be in contact with Dr. Larian personally after surgery (they will get his cellphone number). Personalized care is what helps patients get through this very complicated medical problem.
Consult with Dr. Larian Today!
Dr. Larian is happy to teach patients about the various ways to do minimally invasive parathyroid surgery and help them determine if they qualify for treatment. To schedule a hyperparathyroidism treatment consultation with Dr. Larian, please contact us online or call us today at 310-461-0300.