The body has four pea-sized parathyroid glands in the neck behind the thyroid gland. These glands are responsible for regulating calcium levels in the bloodstream by producing a hormone known as parathyroid hormone or PTH.
Parathyroid adenoma or parathyroid hyperplasia affects the parathyroid glands, so that it overworks, and overproduces PTH. When this occurs, calcium levels can elevate to dangerous amounts in some cases. It is a potentially serious condition if left untreated, impacting most of the organ systems, making them work inefficiently, thus affecting your life expectancy and quality of life.
While the symptoms of hyperparathyroidism might be the same regardless of the cause, understanding the differences between parathyroid hyperplasia vs. adenoma will make a difference in treating the condition.
What is a Parathyroid Adenoma and Parathyroid Hyperplasia?
Parathyroid glands each have millions of cells in them. These parathyroid cells have a calcium sensor (calcium sensing receptor or CaSR) that has a genetically predetermined calcium setting. This means all the parathyroid cells in all four glands normally try to keep the blood calcium level the same number the entire life of a human being.
It only takes one cell to mutate and become abnormal (by changing the setting for the calcium sensor CaSR to a higher calcium number) to throw off the delicate balance of calcium and PTH. The mutating cells can become a parathyroid adenoma or hyperplasia. There are distinct differences between parathyroid hyperplasia vs. adenoma, which determines how they form and how they must be treated.
What is a Parathyroid Adenoma?
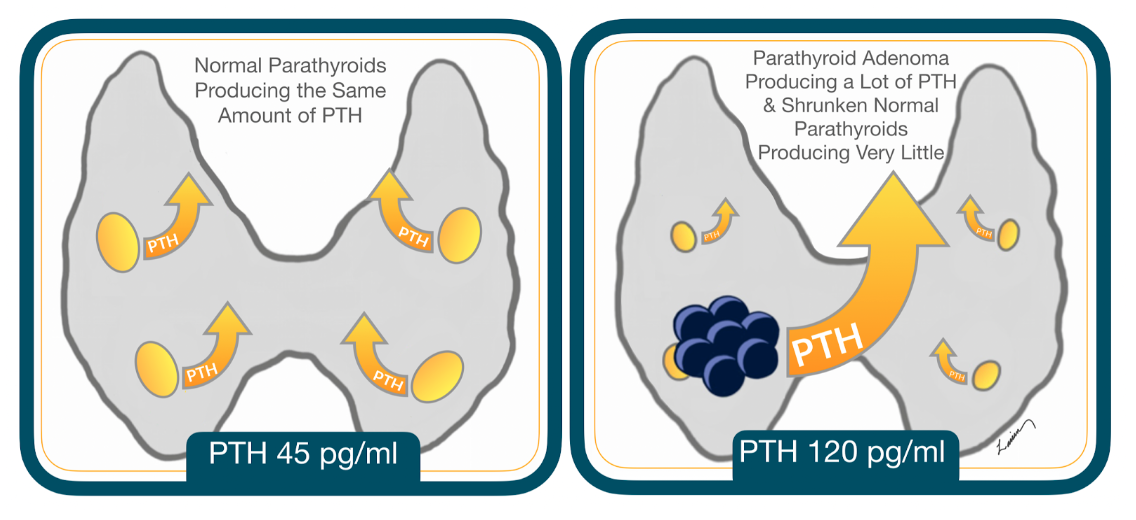
A parathyroid adenoma is a benign tumor that develops inside a single cell of a parathyroid gland. The tumor produces PTH, which increases blood calcium levels. As the tumor gets bigger, the normal cells stop working. Over time, those cells shrink until the normal cells work very little.
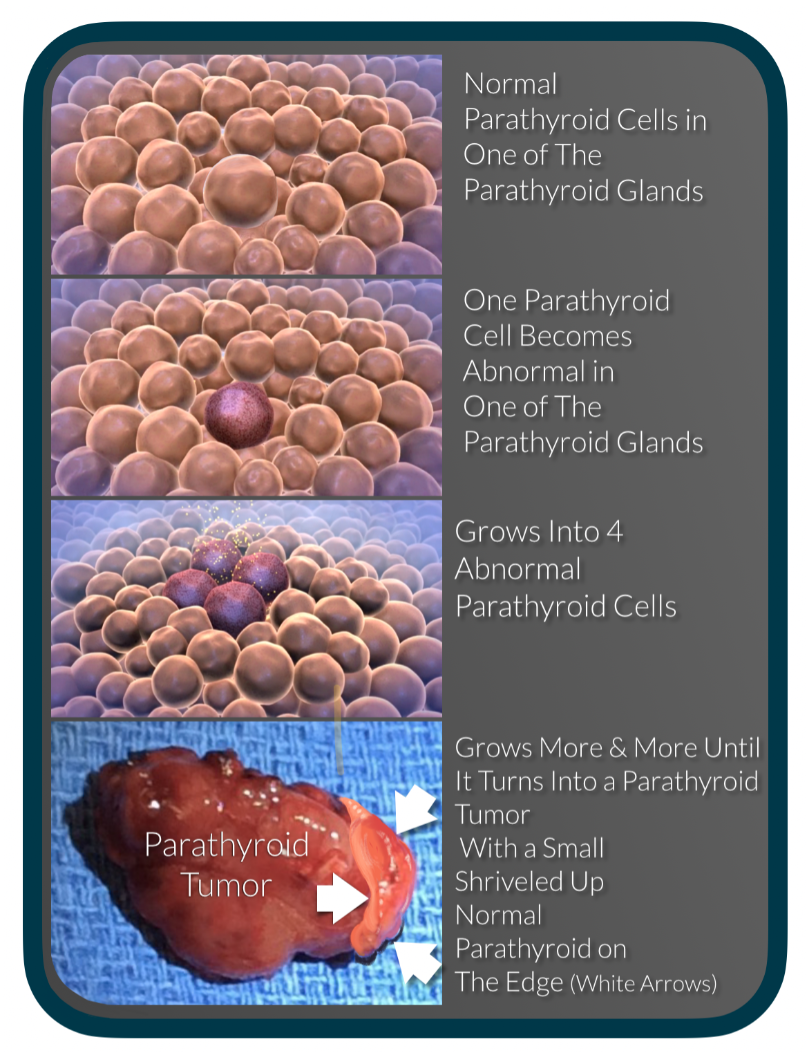
The bigger the adenoma grows, the more PTH it produces. Since the normal cells are no longer functioning, they can’t help regulate blood calcium levels, allowing the PTH to continue to raise calcium to abnormal and potentially dangerous levels.
Rarely, parathyroid adenomas may appear in more than one gland at the same time. They each may produce different amounts of PTH, causing the elevation in calcium. Adenomas in two glands are uncommon (10%), and adenomas in three glands (although they do occur), are exceedingly rare.
What Is Parathyroid Hyperplasia?
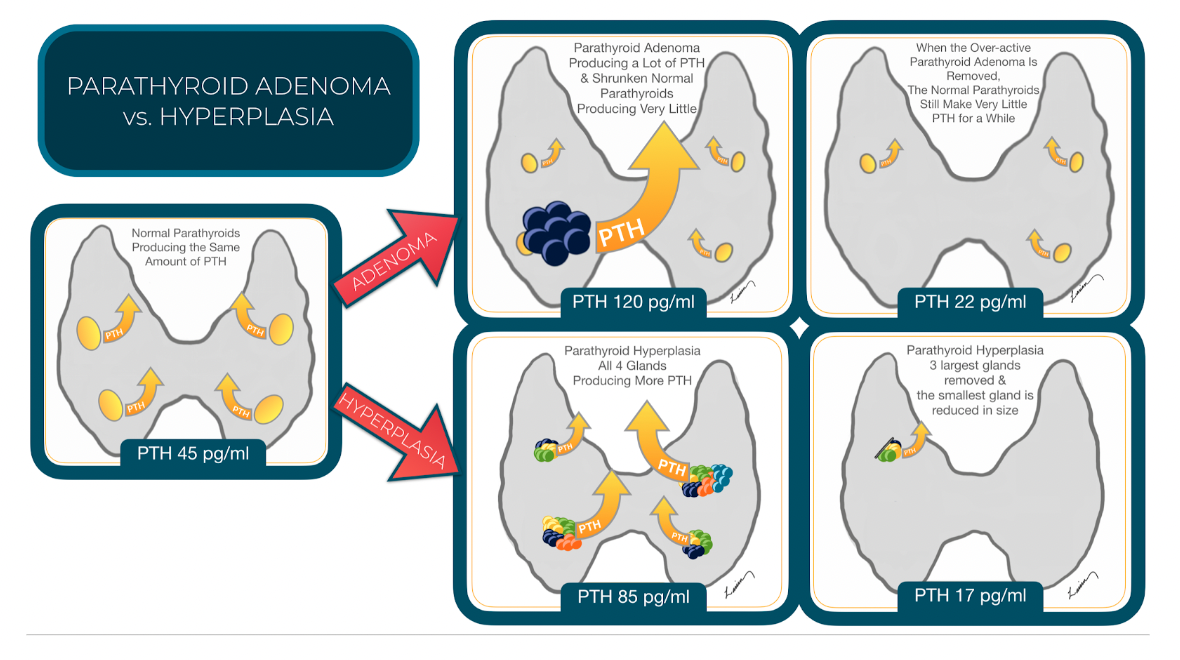
Instead of a single tumor in just one gland, all four parathyroid glands develop abnormal cells, known as parathyroid hyperplasia. The growth of the abnormal cells may vary from gland to gland, with the larger glands producing more PTH. As PTH levels increase, blood calcium levels rise as well.
Causes of Parathyroid Adenoma vs. Hyperplasia
Most parathyroid adenomas appear without any known cause; having said that there is always a mutation in the DNA that is the cause of their development. These mutations can be caused by external toxins or exposures or a genetic mutation that runs in families Radiation exposure is one possible cause. Medication exposure such as Lithium is another cause. Some people also have a genetic predisposition to developing a parathyroid adenoma. If you have a family history of multiple endocrine neoplasia MEN 1 or 2A or hyperparathyroidism, you might be at higher risk.
Potential causes of parathyroid hyperplasia are similar to those of parathyroid adenoma and include radiation exposure and people with a family history of MEN syndromes. Another risk factor could be the long-term use of lithium. Some people develop secondary hyperparathyroidism due to an underlying condition like kidney failure, leading to the appearance of parathyroid hyperplasia.
Symptoms of Parathyroid Adenoma vs. Hyperplasia
The signs and symptoms of parathyroid adenoma vs. hyperplasia are similar and may include:
- Confusion or memory issues
- Ongoing lack of energy
- A general feeling of malaise
- Achy joints or muscles
- Depression and anxiety
- Constipation and stomach aches
- More frequent urination
- Weak bones and frequent fractures
Diagnosis of Parathyroid Adenoma vs. Hyperplasia
Diagnosing hyperparathyroidism is complex enough; distinguishing between parathyroid hyperplasia vs. adenoma is even more challenging. Both of these conditions can present with elevated levels of calcium and PTH or elevated levels of one but not the other. People with hyperparathyroidism caused by hyperplasia generally speaking have lower PTH levels (generally less then 100 pg/ml). But even at these lower PTH numbers of less the 100 pg/ml the chance of a single adenoma is significantly higher at 75%.
Localization studies, such as ultrasound, Sestamibi SPECT, and a 4D CT scan, may also assist in the diagnostic process. An adenoma usually presents with a single enlarged gland on the scans, while hyperplasia may be suspected if all four glands are slightly larger or none show up as enlarged on the scans.
Treatment Options for Parathyroid Adenoma and Hyperplasia
A surgical procedure known as parathyroidectomy is the standard treatment for parathyroid adenoma and hyperplasia. During surgery for parathyroid adenoma, the surgeon removes the parathyroid gland with the tumor. Surgery for hyperplasia involves decreasing the number of abnormal parathyroid cells to restore normal functioning to the remaining parathyroid glands.
Complications and Long-Term Outlook for Parathyroid Adenoma and Hyperplasia
When the parathyroid glands don’t regulate blood calcium levels as they should, the elevated calcium can create complications throughout the body, including:
- Reduced nervous system function, resulting in confusion, memory loss, and fatigue
- Bone weakening that can lead to osteoporosis and bone fractures
- Kidney stones that can lead to kidney damage
- Changes to the blood vessels resulting in high blood pressure
- Issues in the digestive system, such as constipation or acid reflux
- Heart arrhythmias or palpitations
Living With Parathyroid Adenoma and Hyperplasia: Tips and Advice
The long-term effects of parathyroid hyperplasia or adenoma can be devastating. As elevated calcium levels take their toll on various areas of the body, hyperparathyroidism can shorten your life expectancy and affect your quality of life.
Medications can sometimes manage hyperparathyroidism, but they must be taken for a lifetime to keep the condition under control. Surgery is the only “cure” for this disease, whether it is due to a parathyroid adenoma or parathyroid hyperplasia.
Conclusion
Both parathyroid adenoma and hyperplasia can be difficult to diagnose and challenging to treat. Dr. Babak Larian is a board-certified otolaryngologist with expertise in the parathyroid and accompanying conditions. He uses minimally invasive parathyroidectomy (MIP) to treat hyperparathyroidism to preserve surrounding tissue and produce the best possible results.
If you are experiencing symptoms of hyperparathyroidism, you don’t need to suffer alone. The team of experts at the Center for Advanced Parathyroid Surgery can help. Contact us today to learn more about our services, or book your consultation with Dr. Larian.
Parathyroid Adenoma or Hyperplasia FAQ
Do people who have parathyroid adenoma have more symptoms compared to one’s with parathyroid hyperplasia?
Unfortunately, the symptoms for both conditions are the same. You cannot distinguish between the two conditions based on symptoms.
Is parathyroid surgery more challenging for hyperplasia or adenoma?
Parathyroidectomy is usually more challenging for hyperplasia, because all 4 glands need to be found and then the decision needs to be made as to which glands need to be removed. This can be challenging, because some parathyroids that are hyperplastic can appear normal. This is when the surgeon’s experience and expertise becomes very important to achieve good outcomes.
Is it possible to identify an enlarged or overactive parathyroid gland on a sestamibi, 4D CT scan, or ultrasound and still have hyperplasia?
Yes, hyperplasia is often times asymmetric, meaning not all of the abnormal parathyroid glands are the same size. It is possible that of the 4 abnormal hyperplastic parathyroid glands, one may grow to be much larger then the others. And because of this may show up on a scan, making the surgeon think this is the only abnormal scan. That’s why during surgery assessing the functioning of the other 3 glands is important. At the CENTER we prefer PTH testing to make this assessment because it can directly and immediately tell us if another gland, or all other glands are producing too much PTH and need to be removed.
Does the PTH level affect the chance of finding the abnormal gland?
The size of the abnormal parathyroid gland directly correlates the PTH level, so the higher the PTH level the larger the parathyroid adenoma. The larger the gland the easier it is to find by scans and during surgery.
How can a person know that they have hyperplasia before going to the operating room?
The only people that know that they have hyperplasia are the ones that have either familial hyperparathyroidism where all the other members have had hyperplasia (MEN 1 syndrome), or if they have secondary hyperparathyroidism due to kidney failure. In all other circumstances there is no way to be certain. However, we also know that when the PTH levels are high (greater then 150 pg/ml) the chances of hyperplasia is around 5%. And when the PTH is less the 100 pg/ml then the chance is significantly more.