
Secondary Hyperparathyroidism
Secondary Hyperparathyroidism: Diagnosis, Causes, and Treatment
Understanding Secondary Hyperparathyroidism
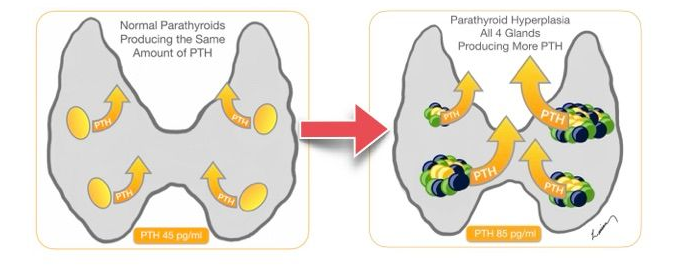
Secondary hyperparathyroidism (SHPT) is a disorder in which the parathyroid glands become overactive in response to chronic deficiency calcium, magnesium, vitamin D etc.. Unlike primary hyperparathyroidism, which is due to a problem within the parathyroid glands themselves, SHPT is driven by an external factor, most often long-standing kidney dysfunction.
In SHPT, all four parathyroid glands usually become enlarged and produce excess parathyroid hormone (PTH) in response to persistent biochemical abnormalities. Over time, this overproduction can cause significant symptoms including bone loss, fatigue, systemic complications and a multitude of other symptoms.
Control Mechanisms of Blood Calcium Balancing
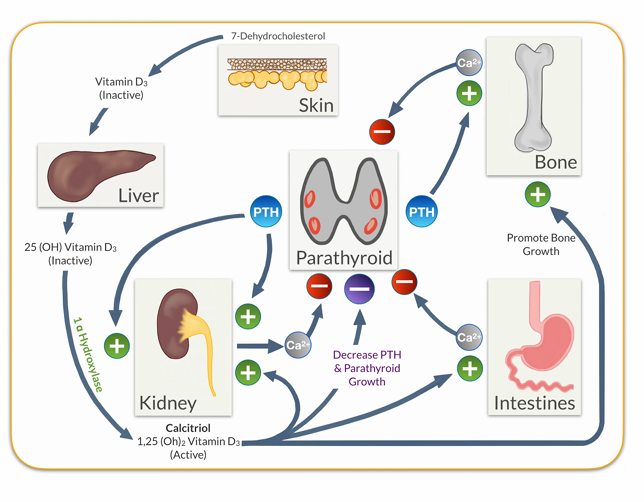
The parathyroid glands are at the center of a blood calcium balancing system. Parathyroid hormone (PTH) activates cells in the bones that cause release of calcium. PTH also instructs the kidneys to bring more calcium back from the urine into the bloodstream. In the kidney it also activates an enzyme called 1Alpha Hydroxylase the turns inactive vitamin D to the active form called Calcitriol. Calcitriol performs two functions in this system: first, it increases the absorption of calcium in the intestines (gut) from 20% to 80%; second, it instructs the parathyroid glands to produce less PTH and not grow. The feedback loops allow the system to keep itself in check and work in harmony.
Causes of Secondary Hyperparathyroidism
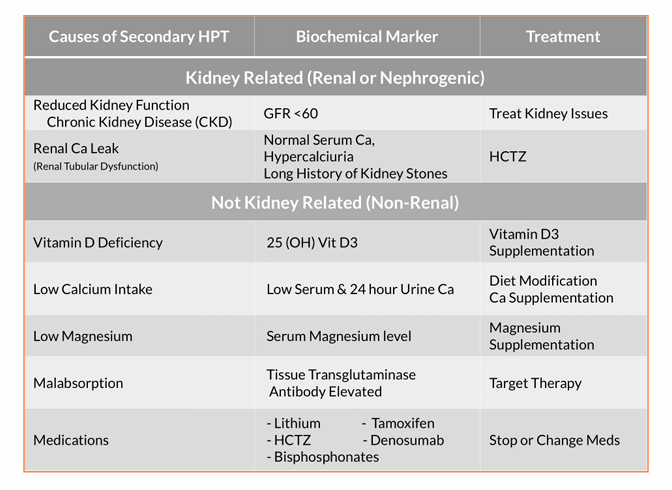
Secondary hyperparathyroidism can result from a variety of conditions that directly or indirectly affect calcium levels. I like to separate out the causes of secondary hyperparathyroidism into two categories: kidney (renal) related or non-kidney related (non renal).
Kidney Related (Renal)
There are two separate and unrelated kidney related SHPT: Chronic Kidney Disease (CKD) & Renal Calcium Leak
Chronic Kidney Disease (CKD)
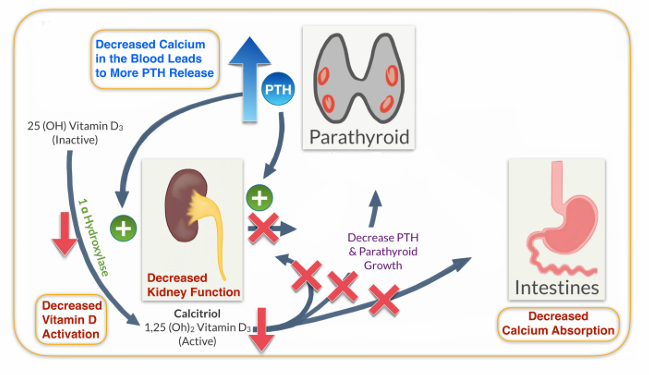
Healthy kidneys convert vitamin D to its active form and help maintain normal levels of calcium and phosphate. In CKD, reduced kidney function leads to:
•Decreased activation of vitamin D (calcitriol)
•Hypocalcemia due to poor absorption of dietary calcium
• Lack of suppression of the parathyroid gland activity & growth
by activated vitamin D
• Impaired phosphate excretion (leading to hyperphosphatemia)
This combination leads to chronic stimulation of the parathyroid glands to produce more PTH in an attempt to restore balance.
Renal Calcium Leak
This is a kidney condition that allows the too much calcium to be filtered out of the blood into the urine. On a 24 hour urine calcium measurement there is excess calcium in the urine. Often times, people affected by this condition will have had multiple kidney stones. However, this does not happen in all instances. The treatment is to use Thiazide diuretics which otherwise known as calcium sparing diuretics.
Not Kidney Related (Non-Renal)
Secondary hyperparathyroidism has several known causes. The most common one is vitamin D deficiency. Vitamin D deficiency leads to decreased calcium absorption from food, causing the parathyroid glands to overwork and overproduce PTH. This hormone helps raise calcium levels in the bloodstream by extracting calcium from bones.
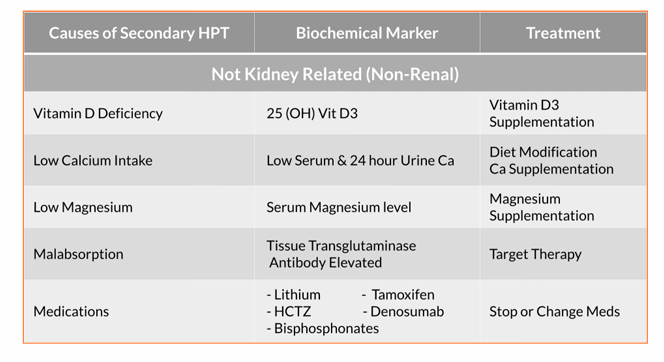
Low dietary calcium also works in the same way, in that there isn’t enough calcium in what the person is eating so again the parathyroid glands overwork. Magnesium deficiency is also correlated to low calcium levels. The impact of magnesium seems to be on the impact it has on the calcium sensing receptor. Intestinal malabsorption, caused by surgery (such as bariatric surgery or intestinal removal) or inflammatory diseases, can lead to decreased absorption of calcium and vitamin D. To overcome this, supplementation can be increased, or sublingual supplements can be used, which don’t require intestinal absorption. Medications – some are listed on the table above. Each work by a different mechanism to interfere with calcium/parathyroid system.
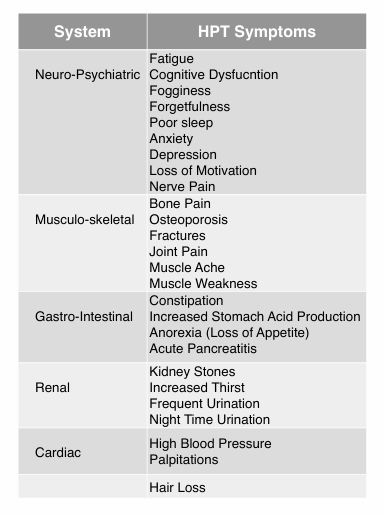
Symptoms
Generally speaking the symptoms can be the same, but the severity has to do with the degree of deficiency and the level of PTH
Diagnosis
The diagnosis is made based on laboratory testing. This requires a deep understanding of all the potential causes of secondary hyperparathyroidism. The natural instinct for many physicians is to say it is caused by vitamin D deficiency, which can be the case. But it is not always the cause or the only cause. So a thorough investigation is warranted along with appropriate treatment and follow up.
Treatment
Parathyoid surgery is NOT the treatment for secondary hyperparathyroidism. Managing the underlying issue should be the primary treatment. In rare cases of kidney failure when the person is on dialysis and PTH levels are very high and causing symptoms surgery may be done.