
Hyperparathyroidism & The Reason For Localization Studies
by Babak Larian | Parathyroid
Hyperparathyroidism is an unusual disease, caused one or more of the parathyroid glands becoming over-active and producing too much hormone (PTH).
Sometimes the gland that is overworking becomes large and produces a lot of PTH. Other times the gland grows only minimally and produces just a little more PTH then expected, but the person’s body maybe sensitive and this little extra PTH can create chaos in the body. So the diagnosis of hyperparathyroidism is almost always made by looking at the relationship between calcium, PTH & vitamin D. The scans are not used to make the diagnosis of hyperparathyroidism, your doctor depends on lab tests to confirm that you have hyperparathyroidism. This is different then most other diseases in the body.
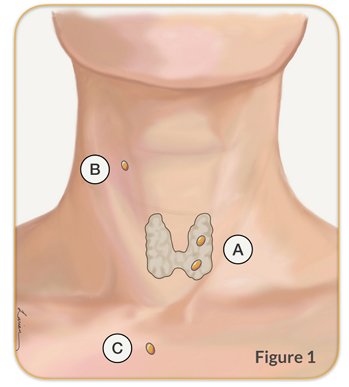
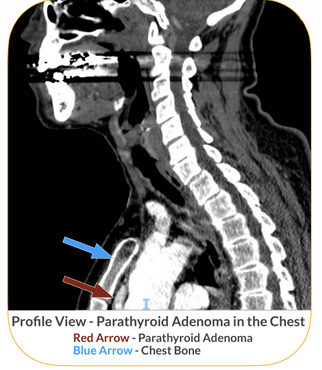
To add to this complexity, parathyroids that develop in the throat of the baby that is in the mother’s belly, and travel down into the neck. This movement of parathyroid can be problematic because only 80% times the parathyroid come to finally be positioned behind the thryoid (position A in Figure 1). The other 20% of times it can travel very little and be in the throat, or travel too much and end up in the chest (position B & C in Figure 1). 3% of people who only 3 parathyroid glands, and 10% have more then 4. So once the diagnosis of hyperparathyroidism is made Dr. Larian will use a parathyroid scan to help identify which parathyroid gland is abnormal, and where it is located. parathyroid glands. This is all done before the day of your surgery so that the doctor to plan your surgery in advance and clearly discuss it with you.
There are many parathyroid scan options, and choosing the right one is sometimes difficult. By working with an expert parathyroid surgeon like Dr. Babak Larian, a patient can undergo a wide range of parathyroid localization studies. Then, if one or more abnormal parathyroid glands is found, Dr. Larian can provide his patient with a personalized treatment plan.
Types of Scans to Locate an Abnormal Parathyroid Gland
In the following sections we will review the various parathyroid localization scans, their advantages and shortcomings. As well as, what is a good strategy to identify the gland. Ultrasound Ultrasound imaging is a reliable way to identify an abnormal parathyroid gland. It uses harmless soundwaves to look at the structures under the skin, including the thyroid, parathyroid, muscles, and blood vessels. An ultrasound should always be the first study to look for an abnormal parathyroid because it is very accurate but does not expose a patient to any type of radiation. When an ultrasound is performed by an expert radiologist, endocrinologist, or surgeon, it has a high likelihood to show an abnormal parathyroid.
In the past decade, ultrasound has become available in many doctor’s offices around the world, and most expert parathyroid surgeons have an ultrasound machine and can immediately do a scan for a patient when HPT diagnosis is confirmed. In this way the patient can start treatment right away.

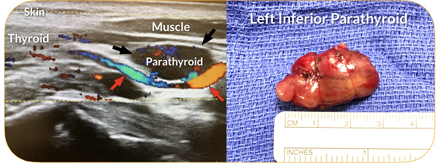
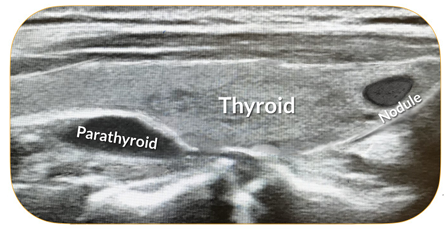
A parathyroid ultrasound can show the exact dimensions of the thyroid gland, enlarged parathyroid glands with the vessels feeding it, carotid artery, lymph nodes, the portion of the thymus that is in the neck, breathing tube (trachea), and the surrounding muscles. The parathyroid adenomas on the 3 ultrasound images show parathyroid adenomas of varying shapes and sizes; and as you can see when the parathyroid is removed in surgery the shape and size directly correlates to finding on ultrasound.
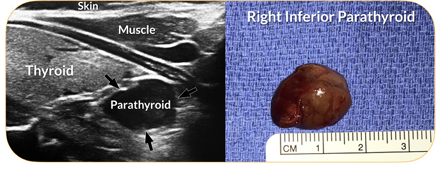
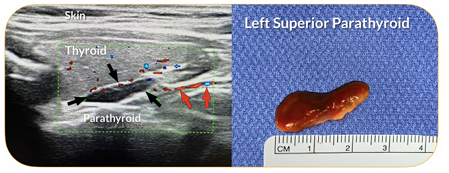
Figure 2-4. Parathyroid adenoma (black arrow), the blood feeding the parathyroid (red arrow). The pictures on the right side show the parathyroid adenoma seen on ultra which was removed during surgery.
Additionally, the surgeon can see exactly where the abnormal enlarged parathyroid is with respect to the thyroid gland, deep to it (superior parathyroid) or in the case of the inferior parathyroid just below the lower end of the thyroid gland. You can also tell how deep the abnormal gland is from the skin, and how big are the blood vessels that are feeding the parathyroid. Another important benefit of ultrasound is that it is by far the best scan to show the thyroid gland itself.
The surgeon can see if there are any nodules in the thyroid gland Figure 5 that need to be addressed at the same time as parathyroid surgery. In the rare case of a parathyroid hiding inside the thyroid gland, the ultrasound would show it. An ultrasound does have its limitations; it cannot be used to show what’s behind bone or cartilage. So, if a parathyroid adenoma is hiding behind the collarbone, chest bone, breathing tube, or voice box, other parathyroid scan options may need to be considered.
All expert parathyroid surgeons perform their own ultrasound to confirm the size and location of an abnormal parathyroid and assess the relationship of the abnormal gland to adjacent structures (thyroid, carotid artery, and recurrent laryngeal nerve), as well as the distance away from the skin.
This information is helpful in planning for parathyroid surgery.
In cases when both an ultrasound and sestamibi scan have been done to identify an abnormal gland in the same area, the accuracy of the findings is greater than 97%.
Dr. Larian repeats the ultrasound in the office to determine the precise location of a parathyroid adenoma so that its exact location is identified to minimize risk during surgery further.
PROS –
Very accurate.
Can show the anatomy of the neck very well and create a roadmap for a surgeon to use to access one or more abnormal parathyroids and avoid important structures.
There is no radiation exposure for a patient.
Can be done in an office.
CONS –
Hard for a surgeon to visualize the anatomy when the procedure is done at another imaging center and not by the surgeon.
Does not show parathyroids that are hidden behind the voice box, breathing tube, chest bone, or collarbone.
Patients that have thyroid inflammation (Hashimoto’s thyroiditis) will often have lots of enlarged lymph nodes that can be confused on a parathyroid ultrasound for an abnormal parathyroid gland.
Sestamibi Scan
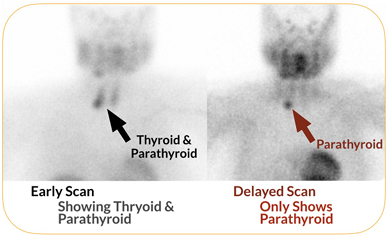
A parathyroid sestamibi scan is an effective way to locate a parathyroid adenoma. In a sestamibi scan, a patient is given a small amount of radioactive dye (sestamibi radiotracer) that becomes quickly absorbed by an abnormal functioning parathyroid gland, as well as the thyroid. In the following few hours, the material leaves the thyroid quickly and the abnormal parathyroid slowly. Next, an initial scan (ideally done within 5 10 minutes of the injection) is compared to a delayed scan (2 hours later) to identify an abnormal parathyroid. The sestamibi is a technical study and can have inaccurate results if it is done at a facility that does not have a lot of experience doing this scan.
Even when the study is done by expert radiologists, sestamibi scans are only able to help locate abnormal parathyroid glands in roughly 85% of cases. When done without expertise, a sestamibi scan can be much less accurate. However, there are times when a parathyroid is either too small or not able to concentrate the sestamibi and won’t show activity on the scan; this does not mean that there is not an abnormal gland, but rather that the gland is not active enough to show on this type of study. It’s also possible that there are multiple minimally active parathyroid adenomas, or that all four glands are abnormal, and each has a low level of activity (too low to be seen on a sestamibi scan).
How a Sestamibi Scan Works: When the parathyroid gland produces parathyroid hormone (PTH), it uses a fair amount of energy. The part of the cell that creates the energy is called mitochondria, and the sestamibi nuclear material is attracted to the actively working mitochondria. The more active the mitochondria is, the more likely it is for sestamibi to attach to it. So, in the situation where PTH levels are high (above 150 pg/dl), sestamibi scans are most likely to be able to help find an abnormal gland. When a patient’s PTH level is less than 100, the likelihood that this scan will show an abnormal gland is low.
The other limitation of sestamibi nuclear material is that not all parathyroid cells have the same number of mitochondria. In the parathyroid glands the oxyphil parathyroid cells have a lot more mitochondria then the chief cells. Therefore, the different types of parathyroid tumor that have different proportions of oxhphil and chief cells will respond differently to the sestamibi injection based, making it a less consistent scan.
As can be seen from the image above, the sestamibi scan does not show detailed anatomy of the person’s neck, but rather the general area of an abnormal gland. Therefore, the parathyroid scan does not give detailed anatomic information that can be used for surgery.
Additionally, you can see activity in multiple salivary glands, some thyroid nodules, as well as other tissues that can be misleading.
PROS –
Very accurate when a patient’s PTH level is high (PTH greater than 150 pg/dl).
Can show parathyroids that are hidden behind the voice box, breathing tube, chest bone, or collarbone.
It can be used to find a gland that is in an ectopic location (unusual spot), as in the upper neck, or down in the chest.
CONS –
Much less accurate if a patient’s PTH level is low (less than 100 pg/dl).
Needs to be done at an imaging center with a lot of experience to ensure accurate results.
Because it uses radioactive material, a patient is exposed to radiation.
It does not give detailed anatomical information, but rather a general location.
The results can be inaccurate if there are thyroid nodules.
SPECT & CT Fusion Scan
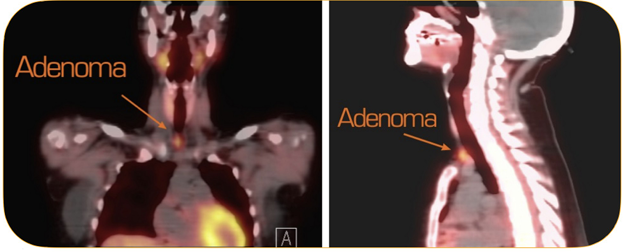
SPECT (single-photon emission computed tomography) is a sophisticated 3D imaging parathyroid scan that uses the same radiotracer as a conventional sestamibi scan, and it fuses the images of a sestamibi scan with a CT scan done at the same time. This combination of images can help pinpoint the exact location of an enlarged parathyroid gland, and therefore, it has greater accuracy than a sestamibi scan performed on its own. However, just as in the sestamibi scan, SPECT imaging must be done at experienced, well-versed imaging centers. Just as in the sestamibi scan, a SPECT scan can miss a parathyroid tumor that is not producing a large amount of PTH. Thus, a SPECT test is not ideal for people who have a PTH level of less than 100. The images shown here point at a parathyroid adenoma (orange dot) in the right inferior aspect of the lower neck, just above the chest bone.
PROS –
Very accurate when a patient’s PTH level is high.
Can show parathyroids that are hidden behind the voice box, breathing tube, chest bone, or collarbone.
It can be used to find a gland that is in an ectopic location (unusual spot), as in the upper neck or down in the chest.
More anatomical detail than a sestamibi scan.
CONS –
Much less accurate if a patient’s PTH level is low.
Needs to be done at an imaging center with a lot of experience for accurate results.
Because it involves the use of radioactive material as well as a CT scan, a patient is exposed to radiation.
Thyroid nodules may affect the results of the scan.
Less anatomical information than a 4D parathyroid CT scan or parathyroid ultrasound.
4D Parathyroid CT Scan
A 4D parathyroid CT scan is a newer imaging study that can be used to locate an abnormal parathyroid, and it is the one of the most accurate localization studies. It works based on the fact that abnormal parathyroid glands have more blood going into and coming out of them, then normal parathyroids and lymph nodes. In other words, the contrast material that is injected into the blood stream for this scan shows blood going in an out the abnormal parathyroid gland quickly.
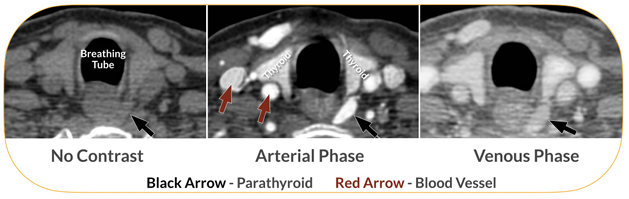
The thyroid gland has good blood flow also but because it likes & uses the iodine in the contrast material, it holds on to it for much longer. The lymph nodes have very little blood flow, so the contrast doesn’t go through them so much. These difference are visible when a CT scan is done at different times after the contrast dye is injected into the bloodstream. This type of scan shows the parathyroid anatomy in great detail along with the blood vessels that are feeding the parathyroid, which helps show an abnormal parathyroid gland and the tissue around it, including the thyroid gland, blood vessels, breathing tube, and esophagus. It will show if an abnormal parathyroid is close to the area of the voice box nerve.

The scan can also show a gland that is not in the normal position (ectopic parathyroid gland), anywhere from the upper neck all the way down into the chest. A 4D parathyroid CT scan is used to identify an enlarged parathyroid better than the other scans mentioned on this page. However, it also exposes a patient to a high dose of radiation. And although we have modified our 4D CT scan protocol to minimize the dose of radiation, radiation exposure is still a consideration, especially in younger patients. We firmly believe this is the study of choice in patients who have had previous parathyroid surgery and had recurrence or persistence of the disease, along with newly diagnosed hyperparathyroid patients who have a negative ultrasound and PTH levels that are below-average.
PROS –
Very accurate.
Can show parathyroid glands anywhere in the neck and chest, even if they are hidden behind the voice box, breathing tube, chest bone, or collarbone.
More anatomical detail than a sestamibi scan or SPECT scan.
More accurate, even when a tumor is small and PTH levels are only slightly elevated.
CONS –
Exposure to radiation.
MRI Scan
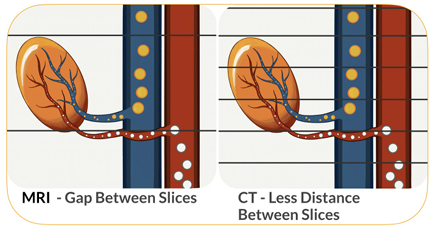
MRI scan is a very good scan to look at internal organs and find tumors. However the distance between slices of MRI are wider then CT scans, a small parathyroid adenoma may not be clearly visible. In fact a smaller flatter parathyroid may be missed between the slices of MRI. However, MRI does not involve exposure to radiation and therefore may be a consideration such as during pregnancy. It does serve as another tool in the armamentarium of a parathyroid surgeon.
Selective Venous Sampling
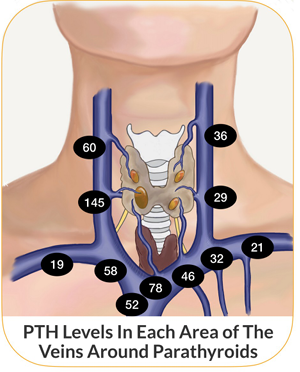
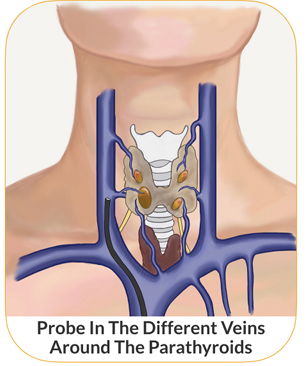
Selective Venous Sampling (SVS) is unique in that we consider to be an invasive localization study. By that we mean that a catheter is placed in the right groin area and then threaded through the vein all the way up to the upper chest and lower neck in the areas surrounding the thyroid. Under X-ray the location of the catheter tip is confirmed by injecting contrast and confirming the tip location. From each separate area here samples of blood are obtained and sent for PTH testing to map out where the highest concentration of PTH is and indicate the general area where the overactive parathyroid may be. This technique is further refined by having the rapid PTH test so that the radiologist can further focus on areas that have higher PTH levels to get more samples and try to more precisely locate the abnormal overactive gland.
It is rare to have this procedure done before any parathyroid surgery has been performed because of it is a very involved & invasive procedure. So it is often used after a person has had a failed parathyroid surgery. But in fact after a previous surgery (in the figure the right superior parathyroid was perilously removed and the blood vessels to it closed) SVS becomes less reliable because the blood vessel anatomy of the area becomes altered; some blood vessels get closed off (ligated) during surgery and new ones form, in time, after surgery. So the blood vessel anatomy becomes more complex and SVS becomes less informative. When we need SVS the most is when it becomes less reliable, so much so that it is now rarely used. An example of a case where I have found it to be helpful is in a person who has had previous total parathyroidectomy and auto-transplantation of a parathyroid into the muscle of the left forearm, who years later develops elevated calcium and PTH. It is not clear if this person has elevation due to over functioning of the autotransplanted parathyroid in the left forearm or if there was a fifth gland in the neck that was not discovered originally. SVS was able to show that high PTH was from the blood vessel coming from the arm and so the surgery could be focused on that area.
PROS –
Very accurate in a person who has never had surgery in the neck.
Can show the general area of the overactive parathyroid gland in the neck and chest.
CONS –
Exposure to radiation.
Not reliable in a person who has had previous neck surgery (previous parathyroidectomy or thyroidectomy).
ADVANCED IMAGING FOR PARATHYHROIDS
18F-Fluorocholine PET Scan (Also Known As: Choline PET Scan)
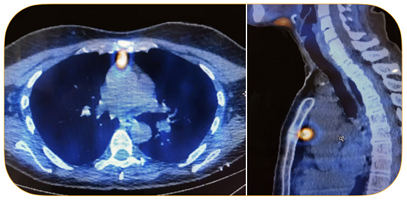
18F-fluorocholine PET scan is a new scan in the world of hyperparathyroidism that shows a lot of promise. 18F-fluorocholine integrates into the surface of newly formed cells in a gland that is more rapidly growing. Additionally, increased PTH in hyperparathyroidism causes more absorption of 18F-fluorocholine into the cell. These two mechanisms seem to act together to concentrate 18F-fluorocholine into the overactive parathyroid gland. Since 18F-fluorocholine is radioactive the scanner will see it as a focus of activity. In the figure above the activity in the ectopic parathyroid gland that is located in the chest can be clearly seen. This was not visible on ultrasound or sestambi/SPECT scan.
There are certain limitations to this scan as well. It is not specific to the parathyroid gland, other types of tumors, cancers and inflammation will show activity on this type of scan. In fact, it has been mainly used for prostate cancer. It is also not readily available; there are only a few hospitals that perform this scan in the United States and around the world.
PROS –
Very accurate.
Can show parathyroid glands anywhere in the neck and chest.
More accurate, even when a tumor is small and PTH levels are only slightly elevated.
CONS –
Exposure to radiation although a lower dose then other scans.
Only available in a few hospitals.
4D Dynamic MRI Scan
A 4D Dynmanic MRI scan is very similar in nature to 4D Parathyorid CT scan. The idea behind it is that overactive parathyroid glands have more blood flowing through it and there the contrast injected in the MRI will go in and out of the gland rapidly which can be seen on MRI. There have been several studies indicating that this technique maybe as accurate as 4D CT scan, without exposure to radiation. It certainly is a very good option for patients that are allergic to iodine based contrast used for CT scans. It does have the drawback as mentioned before that a small parathyroid may be missed in the gap between the slices of MRI, nonetheless it is a promising option.
Localization Scan Strategy
An ultrasound is usually a very accessible and inexpensive study to identify the abnormal parathyroid, it can also show if there are nodules in the thyroid that need to be treated during surgery. Most hospitals and imaging centers have good ultrasound machines. If ultrasound is not successful in finding the abnormal parathyroid, then we recommend the patient try to get a 4D parathyroid CT scan next. Although this scan is not always available, it is not because it requires a special CT scan machine. Rather it requires that the radiologist use a special timing after injecting the contrast. If your local imaging center is not used to doing this, you can refer them to the following article to get the protocol. If ultimately 4D CT scan is not able to be done, then a Sestamibi-SPECT scan is the next best choice. If both the ultrasound and 4D CT are not successful this may be considered, specially if PTH levels are above 100-150 and the chance of hyperplasia is considered to be low (no family history of HPT etc…)
Parathyroid Scan FAQ
Dr. Larian understands that patients often have a lot of questions about the imaging tests required for locating parathyroid tumors and that the choice of which scan to get can be confusing. He has answered some common questions for you below to help you through this process.
- Can localization scans help make the diagnosis of hyperparathyroidism?
No, the diagnosis of HPT is made by laboratory findings. The scan is only to help identify where the abnormal gland is located. - Which scan should be the first choice?
Ultrasound should always be the first choice because it only uses soundwaves. There is no radiation involved during an ultrasound, too.
- Should I be concerned about radiation exposure?
Many patients express some concern in regards to being exposed to radiation for parathyroid scans. First, the decision to proceed with one of the studies that uses radiation (sestamibi, SPECT, or 4D CT scan) should only be made if the ultrasound is not successful in finding the abnormal parathyroid. Having said that, the dose of radiation in sestamibi, SPECT, and 4D CT scans is low and generally not harmful. Knowing the exact location of the abnormal parathyroid allows a surgeon to perform a minimally invasive focused surgery, which limits scarring, trauma to tissue under the skin, and recovery time. This outweighs the disadvantage of radiation exposure of a scan. - Where do I go for a sestamibi SPECT scan?
If we are treating a patient who lives in the Los Angeles area for a parathyroid disorder, Dr. Larian will send the patient to one of the local hospitals with great expertise in performing SPECT sestamibi scans. If a patient cannot get to LA for the scan, we will recommend a reputable medical center that performs this type of scan on a regular basis, which is usually the larger hospitals. You have to ask the imaging center how often it performs a sestamibi scan and what is their success rate in identifying an abnormal gland. A success rate of less than 70% is not acceptable. - Do all parathyroid surgery patients need a sestamibi SPECT scan?
No, only patients who have a negative ultrasound study and have a PTH level that is higher than 150 pg/dL should undergo a sestamibi SPECT scan. Or if the person has done multiple other scans that have been unsuccessful. - When would you choose a 4D parathyroid CT scan over a SPECT scan?
When a patient has had a negative or equivocal ultrasound study at the CENTER we usually recommend a 4D parathyroid CT scan. We feel this scan is more successful then others, especially when the PTH is lower. The chance of a sestamibi or SPECT scan being positive when a patient’s PTH level is less than 100 pg/dL is significantly lower because the abnormal gland is not very active and not producing a lot of PTH. This decreases the attraction of the parathyroid to the sestamibi radiotracer and makes the radiotracer less likely to attach to it and show up on the scan. - Is a high-resolution CT scan of the neck and upper chest the same as a 4D parathyroid CT scan?
No, a 4D parathyroid CT scan is a specialized form of a high-resolution CT scan. It not only looks at a more detailed and precise imaging of the neck and upper chest (smaller gap distances between the slices) but also at different time points after injecting the contrast dye. This allows the 4D scan to see the contrast in how blood flows through tissue to distinguish between lymph nodes, thyroid tissue, and overactive parathyroids. The ability to tell these tissue apart from each other is helpful, because on a regular CT scan, they can look the same. - Can a single parathyroid scan be used to identify an abnormal parathyroid gland?
At the CENTER, Dr. Larian is able to find a great majority of abnormal parathyroids on ultrasound alone. A parathyroid surgeon performing an ultrasound has the added advantage of being to able to compare ultrasound findings to what they see in surgery; this in time gives the parathyroid surgeon an exceptional amount of insight. A minority of patients require multiple localization studies to identify an abnormal parathyroid gland. Each localization study is used to help create a personalized treatment plan for a patient, and ultimately, ensure that a patient can alleviate HPT symptoms. - If a parathyroid scan shows that a patient is dealing with an abnormal parathyroid gland, what happens next?
Once an abnormal parathyroid is identified, then a focused surgery to remove the abnormal parathyroid can be done. - What will happen if a parathyroid scan comes back negative?
Negative results from a localization study only means the abnormal gland was not visible on that particular scan, NOT that the person does not have hyperparathyroidism. Additional tests need to be find the abnormal parathyroid gland. - When do the results of a parathyroid gland scan become available?
Ultrasound done in the office will give you results immediately. Otherwise scans done at imaging centers/hospitals will give results in 1-2 days. Fortunately, at CENTER, Dr. Larian is able to get results of scans from the imaging center or hospital we use on the same day, and in fact can bring up the images and review them with the patient right away. - How long does it take to complete a parathyroid gland scan?
The length of time required to complete a parathyroid gland scan varies from a few minutes for ultrasound & CT scan, to 45 minutes for MRI, and hours for Sestamibi SPECT scan.
Contact The CENTER For Advanced Parathyroid Surgery Today
Dr. Larian is an experienced parathyroid surgeon in Los Angeles with over 2 decades of experience in hyperparathyroidism surgery. unique knowledge in parathyroid gland diagnostic testing and the meaning and ramifications of parathyroid gland testing for patients suffering from HPT. Dr. Larian is happy to perform localization studies to help a patient diagnose HPT. And if a patient is dealing with HPT, Dr. Larian can provide a custom treatment recommendation. If you feel as though you may be experiencing parathyroid problems and would like to speak with an expert parathyroid surgeon today, we encourage you to contact our CENTER by calling 310.461.0300 to set up an initial consultation.